Designed to provide business leaders and their key advisors with the knowledge and insight they need to grow and sustain successful digital health initiatives, we are pleased to present The Law of Digital Health, a new book edited and authored by McDermott’s team of distinguished digital health lawyers, and published by AHLA.
Visit www.mwe.com/lawofdigitalhealth to order this comprehensive legal and regulatory analysis, coupled with practical planning and implementation strategies. You can also download the Executive Summary and hear more about how Digital Health is quickly and dynamically changing the health care landscape.
What if you didn’t have to take time out of your day to see a physician in person when you needed a prescription? What if a diagnosis could be delivered over video chat? What if your psychiatrist was available at the press of a button or swipe on your screen?
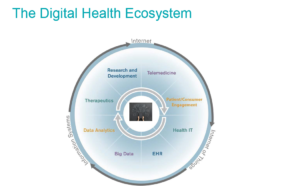
These options are fast becoming a reality, as telehealth (or telemedicine) continues to take hold in a health care system that is desperate for increased efficiency and higher quality outcomes. And while telehealth offers exciting new possibilities in terms of convenience and access for patients, it also poses new regulatory challenges for industry stakeholders still learning the new rules of the game in today’s digital health ecosystem.
The Chronic Care Act
One of the biggest drivers of change in the industry right now is the Chronic Care Act. Last month, as part of the House and Senate budget deal to fund the government through March 23, legislators included the Creating High-Quality Results and Outcomes Necessary to Improve Chronic (CHRONIC) Care Act of 2017, which will increase reimbursement for a lot of different telemedicine programs.
For example, if you went to a rural hospital and they didn’t have a stroke neurologist and you were having a stroke, you would have an ED doctor with no stroke specialty diagnosing you—not an ideal situation. With telemedicine, it’s now possible for rural doctors to consult with specialty doctors at renowned sites, which the government will fund thanks to the Chronic Care Act. (more…)
The explosion in digital health solutions that connect consumers with licensed health care providers (e.g., nurses, nutritionists, physicians) and laypersons who have certain informal training (e.g., wellness guide, lifestyle coach, outreach partner) has the potential to blur the lines between what constitutes the practice of a licensed health care profession and what does not (usually because the service is intended to be merely informational or educational). Why does it matter which side of the line a particular service falls on? If a service is one that is delivered by a licensed health care professional, there are various state laws and regulations that may govern the activity, and different potential causes of action that may apply in the event a consumer/patient is injured in the process.
If a digital health solution connects a consumer to an individual who is engaged in an activity that is normally performed by a licensed health care professional, state laws and regulations governing health care professionals likely apply.
As background, state professional boards regulate individuals who deliver health care services to the public (e.g., nursing, psychology, medicine, phlebotomy). What falls within the definition of a specific health care service can be very broad and varies state to state. (more…)
This past fall, after months of speculation, President Trump declared the opioid crisis sweeping the United States a national public health emergency. Upon the president’s declaration, Acting Health and Human Services Secretary Eric D. Hargan made a formal declaration under Section 319 of the Public Health Service Act, making available an exception to the Ryan Haight Online Pharmacy Consumer Protection Act of 2008 (the Haight Act) that would allow providers to prescribe controlled substances using telemedicine without first conducting an in-person visit. Currently, the Haight Act restricts the ability of a provider to prescribe controlled substances using telemedicine without first conducting an in-person examination, unless an exception applies. For a detailed discussion regarding the Haight Act and the restrictions on the use of telemedicine to prescribe controlled substances within the context of the treatment of opioid addiction and mental health generally, our latest article addresses the opioid crisis and access to mental and behavioral health providers.
The declaration of a public health emergency allows the US Drug Enforcement Agency (the DEA) to remove the restriction of prescribing controlled substances using telemedicine for the treatment of opioid addiction, but the DEA has not promulgated any rules or guidance on the subject. The lack of development has drawn the interest of Senators Claire McCaskill, Lisa Murkowski, and Dan Sullivan. The senators, in a January 30, 2018, letter to Robert Patterson, the acting administrator of the DEA, note that the restriction on the use of telemedicine from prescribing addiction treatment medications continues to have a harmful impact on rural Americans, citing specifically to Missouri, where 98 out of its 101 rural counties lack a licensed psychiatrist. In this letter, the senators call on Mr. Patterson to expedite the rulemaking process to create a special registration process to permit the prescription of opioid-based medication-assisted addiction therapies via telemedicine without first performing an in-person visit.
McDermott Will & Emery LLP will continue to monitor whether progress is made to develop this expedited rulemaking process and report updates on this blog.
The opioid epidemic is making the United States acutely aware of the horrors of substance abuse disorders and the limited means of treating the individuals suffering from addiction. Rural America is among the places hit hardest by opioid addiction while also having limited access to mental and behavioral health providers.
Telemedicine offers a viable solution to provider shortages, particularly with an eye toward mental health care professionals. Although telemedicine alone will not remedy the shortage of psychiatrists in the United States, the technology does possess the capability of greatly increasing access to them; however, a large driver of psychiatric care is provided through pharmaceutical treatments.
The ability for providers to prescribe pharmaceuticals, particularly controlled substances, to patients the provider has not seen in person is limited by the Ryan Haight Online Pharmacy Consumer Protection Act of 2008 (Haight Act). The relevance of the Haight Act, a law that went into effect almost nine years ago, has been revitalized, but the opioid epidemic and advances in psychiatric treatment are now demonstrating the law requires clarification through amendment to improve access to pharmaceutical treatments and, in turn, increase access to mental health care.
On February 9, 2018 after a brief shutdown, Congress passed and President Trump signed the Bipartisan Budget Act of 2018, a two-year budget agreement that includes funding for the operation of the federal government until March 23, 2018. The law includes significant health care policy changes impacting Medicare, Medicaid and other federal health agencies. In addition to raising federal spending caps enacted in the Budget Control Act of 2011, this legislation includes additional spending for health care priorities. Here we break down some of the changes affecting telehealth.
Expanded Access to Telehealth Stroke Services
The new law expands, beginning in 2019, the ability of patients presenting with stroke symptoms at hospitals or mobile stroke units to receive a timely telehealth consultation with a neurologist in order to determine the best course of treatment. The provision eliminates the current geographic restriction that limits originating sites to rural areas, meaning distant site providers delivering telestroke services could receive a professional fee for delivering the consultation to patients located anywhere in the United States, provided that the other Medicare telehealth coverage requirements are satisfied (e.g., type of provider, type of technology). (more…)
Stephen Bernstein, global chair of McDermott’s Health Industry Advisory Practice Group, sat down with This Week in Health Innovation at the J.P. Morgan Healthcare Conference in San Francisco.
Stephen and Dr. Andre Berger, CEO of National ACO, discussed the role of advancing technologies in enhancing collaboration between key players in digital health—including doctors, heath plans, investors, and consumers and patients—and how digital health is necessary for improving care delivery and managing costs.
Blockchain is rapidly becoming the focus of conversations regarding health care disruption, and for good reason. What started out as a means for cryptocurrency is now making waves in a variety of industries, set to revolutionize how data is stored and shared.
The inability to easily and securely store and share data has long been a burden on the health system. Blockchain poses a solution to that through encryption and highly advanced technological assets which open the doors to health care innovation. Today we see blockchain being used with electronic health records (EHRs) so that a patient’s medical history is easily accessible to him/her, as well as his/her doctors, insurance providers, etc. It’s also providing the “how” in implementing value-based payment agreements, which link payment to performance of a drug or medical device. Blockchain is currently being used both in the private and public sectors, including the FDA and the CDC. While the full potential of this new technology is not yet known, the industry seems eager to find out.
Ahead of this year’s J.P. Morgan Healthcare Conference, we sat down with Lee Schneider, our top blockchain thought leader, to talk specifically about how this new technology is revolutionizing (or has the potential to revolutionize) the health care space. (more…)
Disruption of traditional health care is inevitable and poses a central challenge for health care governance. While the size and complexity of the health care industry have slowed the process of business disruption, its high costs and lack of convenience make it highly vulnerable to innovative, nontraditional competitors.
To make sure boards are well-prepared to address this challenge, McDermott Will & Emery and Kaufman Hallhave partnered on a new thought leadership series designed to help you identify the signs of disruption, learn how to prepare your organization, and understand the implications for health care governance.
Listen to Surviving Disruption Podcast, Episode 1: The Signs of Disruption.
Download Is Your Organization Disruption Ready? Questions to Assess Preparedness.
View our Top 5 Business Disruption Considerations for Corporate Governance infographic.
Watch our Behind the Scenes: The Making of the Surviving Disruption Podcast Series video.
Subscribe to the Surviving Disruption podcast on iTunes, SoundCloud and Pocket Casts, and keep an eye on the Resource Center for Episode 2: The Path Through Disruption and Episode 3: A Governance Foundation, being released on December 27 and January 10.
President Trump declared the opioid addiction epidemic a public health emergency yesterday. The White House made it clear that this declaration would allow officials to remove barriers to the prescribing of controlled substances via telemedicine, which would permit DEA registered providers to prescribe anti-addiction medications, such as Naloxone, to patients in need without first performing an in-person exam.
As background, the Ryan Haight Online Pharmacy Consumer Protection Act of 2008 (the Haight Act) requires a telemedicine provider who is prescribing a controlled substance to a patient to perform an in-person medical evaluation of the patient prior to prescribing a controlled substance, unless one of the narrow telemedicine exceptions set forth in the Haight Act applies. Additional information on the Ryan Haight Act and the implications of this declaration can be found here.
There are many important questions remaining to be answered, including whether any funding will be available to support the implementation of this declaration and whether the declaration will be renewed upon its expiration in 90 days. The answers to these questions are important to healthcare providers who will need to invest resources and time into developing telemedicine programs to reach more substance use disorder patients, which may take longer than 90 days to implement.

 Subscribe
Subscribe